CUHK unveils two distinct subtypes of rheumatoid arthritis structural joint damage in the world’s longest MRI follow-up study: calling for early MRI-based detection to reduce risk of permanent disability
The Chinese University of Hong Kong (CUHK)’s Faculty of Medicine (CU Medicine) has pioneered the world’s longest-ever advanced magnetic resonance imaging (MRI) study of patients with rheumatoid arthritis (RA), covering an eight-year period. The study revealed two distinct patterns of structural joint damage in patients with early rheumatoid arthritis - progressive and non-progressive structural damage patterns - which cannot be detected by usual X-ray examination. This breakthrough clearly defines two distinct subtypes of RA structural joint damage with MRI as a critical tool for early detection. It paves the way for potentially treating these two subtypes differently with a view to minimising irreversible joint damage and disability. The findings have been published in the prestigious international medical journalEuropean Radiology.

Featured are (left) Professor Tam Lai-shan, Chair Professor and Head of the Division of Rheumatology in the Department of Medicine and Therapeutics; and Professor James Griffith, Chairman of theDepartment of Imaging and Interventional Radiology, both from CU Medicine.
RA-related inflammation causes structural joint damage
RA is a common autoimmune systemic disease affecting over 70 million people worldwide, including up to 30,000 people in Hong Kong. It is usually diagnosed between the ages of 30 and 50 years and affects women three times more commonly than men.
RA is also an inflammatory disease that can lead to structural joint damage, causing joint pain and stiffness, particularly in the small joints of the wrists, hands, and feet which may be associated with progressive joint deformity, and irreversible loss of function without timely intervention.
Two new structural damage patterns help predict disability risks within eight years
Researchers conducted the longest MRI-based follow-up study by tracking 81 early RA patients for eight years, far surpassing the previous longest MRI follow-up study of two years. All participants had symptoms for less than 24 months and underwent MRI scans to assess inflammation and structural joint damage at baseline, after the first year, and after the eighth year.
The research uncovered two distinct RA progression pathways, related to how the disease will progress over time due to inflammation. About two-thirds of patients had a non-progressive structural damage pattern (the “non-progressive subgroup”), with only minimal or mild structural damage on MRI at initial presentation. These patients did not develop further structural deformity throughout the eight-year follow-up period.
In contrast, the remaining one-third had a progressive structural damage pattern (the “progressive subgroup”). These patients showed moderate to severe joint destruction on their MRI at initial presentation and continued to deteriorate over time despite receiving immune-modulating drugs. By the eighth year, functional impairment was twice as severe in the progressive subgroup as the non-progressive subgroup. The presence of significant structural deformity in the progressive subgroup even at initial presentation indicates that this particular subgroup of patients is already being diagnosed too late - highlighting a crucial challenge in RA management.

Non-progressive structural damage group showed mild structural damage at initial presentation (with a score of about 15), with no significant deterioration over the following eight years. In contrast, progressive structural damage group already exhibited moderate to severe structural damage at baseline, followed by drastic and irreversible deterioration thereafter.
Professor James Griffith, Chairman of theDepartment of Imaging and Interventional Radiology at CU Medicine said: “Critically, both groups of patients had experienced symptoms for the same duration before their initial MRI but their structural damage patterns were entirely different. This is the first clear evidence that RA comprises two distinct subtypes, one with progressive structural deterioration and one without. MRI enables the two structural damage subtypes of patients to be identified by doctors at an early stage, helping to predict, with a high level of confidence, whether the patient is likely to develop structural damage in the long-term.”
MRI helps catch aggressive RA early with high diagnostic precision
The level of structural damage detected by MRI at diagnosis is a powerful predictor of the long-term structural damage caused by RA. Structural damage can be overlooked without using MRI as X-rays are not sensitive at revealing structural damage. According to the research findings, MRI demonstrated significantly higher accuracy in predicting structural damage, with an area under the curve[1] (AUC) score exceeding 0.8 (with 1.0 being the highest score), approaching near-perfect classification of structural damage by the eighth year. Clinical, serological and radiographic assessments only achieved AUC scores of up to 0.6.

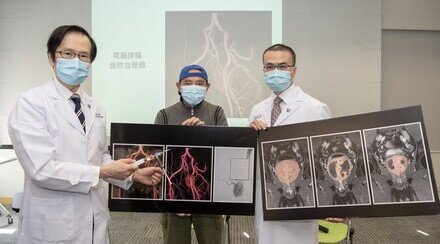
Through the world’s longest-ever advanced magnetic resonance imaging (MRI) study of patients with rheumatoid arthritis, CU Medicine discovers, for the first time, the non-progressive and progressive structural damage patterns. The discovery highlights MRI outperforms X-ray examination in identifying structural damages, helping doctors predict the risks of severe joint deformity and disability within eight years.
Professor Tam Lai-shan, Chair Professor and Head of the Division of Rheumatology in the Department of Medicine and Therapeutics at CU Medicine, added: “The reason for this distinction to remain hidden until now is that high-resolution imaging like MRI, which is far more sensitive than
X-rays at revealing early structural damage such as erosions, joint space narrowing, and inflammation such as synovitis, tenosynovitis, and bone edema, had never been used in such a long-term study. Understanding the mechanisms that differentiate these subtypes may pave the way for more advanced, personalised, and effective precision therapeutic strategies.”
The study has significant implications for clinical practice and future research. Researchers recommend performing high-resolution MRI on RA patients at diagnosis to identify the progressive subgroup early, enabling suitable intervention to slow or halt disease progression – and helping to minimise disability and long-term functional impairment in RA patients.
[1] AUC refers to area under the curve, which is a metric used to assess overall diagnostic accuracy. It ranges from 0.5 (no better than chance) to 1.0 (perfect discrimination). The higher the AUC, the more accurate the evaluation is.