CUHK and PWH multi-disciplinary aortic team saved an extremely rare case of aortic dissection complicating twins pregnancy
In June 2024, a pregnant woman carrying twins was admitted to the Prince of Wales Hospital (PWH), due to sudden chest pain and was diagnosed with aortic dissection. Since it was an extremely rare and emergent case, The Chinese University of Hong Kong (CUHK)’s Faculty of Medicine (CU Medicine) and PWH formed a multidisciplinary team involving cardiac surgeons, obstetricians, anaesthesiologists and intensivists to urgently discuss the optimal treatment. Eventually, the team successfully performed an aortic root replacement surgery, also known as a Bentall procedure, with cardiopulmonary bypass support and in utero protection, saving the lives of mother and babies. Due to case’s rarity and clinical importance, a report was published in an international medical journal of cardiothoracic surgery The Annals of Thoracic Surgery.

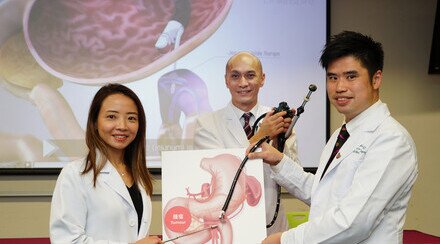
From left: Dr Clarence Chan Hui-wah, Resident of the Division of Cardiothoracic Surgery at PWH; Professor Liona Poon Chiu-yee in the Department of Obstetrics and Gynaecology at CU Medicine; Professor Randolph Wong Hung-leung in the Division of Cardiothoracic Surgery in the Department of Surgery at CU Medicine; Dr Lai Man-ling, Deputy Chief of Service of the Department of Anaesthesia, Pain and Perioperative Medicine at PWH; and Dr Henry Wong Man-kin,Assistant Professor (Clinical) of the Department of Anesthesia and Intensive Care at CU Medicine.
Increased cardiac load raises the risk of aortic dissection in late pregnancy
Aortic dissection[1] is a rare but imminently life-threatening cardiovascular condition in which a tear occurs in the inner layer of the aorta and blood rushes through the tear, causing the inner and middle layers of the aorta to dissect and create a false lumen. This affects normal blood supply and can lead to aortic rupture or organ ischemia in severe cases. During pregnancy, women experience an increase in blood volume, significantly raising the pressure on the cardiovascular system. If accompanied by pregnancy-induced hypertension, this can cause weakening of the aortic wall, increasing the risk of aortic dissection, which is most common in the third trimester (the last three months of pregnancy) and in the postpartum period (six to eight weeks after delivery). The global incidence is four to seven per million pregnancies, with intraoperative mortality rates for both the mother and fetus reaching as high as 20%.

Professor Poon says women experience an increase in blood volume during pregnancy, significantly raising the pressure on the cardiovascular system. The risk of aortic dissection for pregnant women is four times of the general population.
Professor Liona Poon Chiu-yee in the Department of Obstetrics and Gynaecology at CU Medicine and Honorary Consultant in the Department of Obstetrics and Gynaecology at PWH , said: “Aortic dissection during pregnancy represents a rare but extremely complex and challenging case for doctors. Therefore, it is the utmost importance for a multidisciplinary team to work together for the best outcome. The surgical approach depends on gestational age, balancing the risks to mother and fetus. For gestation age of 26 weeks or above, the guidelines suggest a single-stage ‘deliver-then-repair’ approach. Given that the survival rate is very low for those fewer than 26 weeks of gestation in this circumstance, guideline suggests a Bentall procedure with subsequent delivery.”
The CUHK-PWH team finished the Bentall procedure in four hours 35 minutes and the woman gave birth to healthy twins six weeks later
The 36-year-old woman with 25-week-gestation twins presented with chest pain radiating to her back. A bedside echocardiogram in hospital showed her aortic root dilated from a normal diameter of 3cm to 5cm with severe aortic valve regurgitation. She was diagnosed after a contrast-enhanced computed tomography aortogram with Standard type A aortic dissection, a life-threatening condition for her and her twins.

Ms Chen says she felt very helpless when she first learnt about having aortic dissection and that both her babies and herself were in life-threatening condition. She later calmed down and decided to trust her doctors. Babies’ health and safety were her priorities. She is very thankful that the team did the very best to safeguard the three lives.
CU Medicine and PWH formed a multidisciplinary team involving cardiac surgeons, obstetricians, anaesthesiologists and intensivists to handle the case. They discussed with the patient’s family and then came up with a through surgical plan. The team decided to conduct a Bentall procedure with cardiopulmonary bypass support, with in utero protection.
Professor Randolph Wong Hung-leung in the Division of Cardiothoracic Surgery of the Department of Surgery at CU Medicine and Team Head of the Division of Cardiothoracic Surgery at PWH, said, “Cardiopulmonary bypass is used to temporarily replace the patient's own heart and lung functioning during a Bentall procedure. The traditional procedure involves systemic cooling to protect the patient from ischemia-induced injury and to reduce metabolic demands. Considering that the fetuses were at risk of life-threatening conditions due to hypothermia or cardiac arrest, and to ensure adequate uterine blood flow to supply oxygen to the twins, we decided to perform the surgery without systemic cooling, while regularly conducting fetal echocardiograms to ensure their stability.”

Dr Lai (right) says the operation was not just about one patient, but a mother of twins and that they had to take the safety concern for all of them into consideration when designing the procedures, including the plans for anaesthesia and vital measurements.
Dr Lai Man-ling, Deputy COS of the Department of Anaesthesia, Pain and Perioperative Medicine at PWH and Clinical Associate Professor (Honorary) in the Department of Anesthesia and Intensive Care at CU Medicine, said: “The patient was positioned in a left lateral tilt to avoid inferior vena cava compression and put under general anesthesia. We continuously monitored the patient’s heart condition with echocardiography before and after the cardiopulmonary bypass. The team also needed to precisely calculate the dosage of anesthetics to maintain the patient’s blood pressure at a higher level and to accurately control her coagulation indices.”
The operation lasted 4 hours 35 minutes. The patient made an uneventful recovery. She was discharged from the intensive care unit on Day 4 after surgery and highly-dependency unit on Day 8, discharged from hospital on Day 17. She successfully sustained her pregnancy for six more weeks and delivered healthy twin at 31 weeks.

Professor Wong says they chose to use a mixed biological heart valve and synthetic graft for the aortic root replacement instead of the traditional large vessel segmental suturing, successfully saving cardiac arrest time to lower the risk of complications.
Professor Wong said: “It is extremely rare that we have to save three lives in one single surgery. The complexity of both the surgery and the anesthesia demanded a highly experienced multidisciplinary team. Postoperative care also needed be considered to ensure the recovery of the patient and the subsequent delivery. The entire surgery was time-sensitive; we chose to use a mixed biological heart valve and synthetic graft for the aortic root replacement instead of the traditional large vessel segmental suturing, successfully saving more than 15 minutes of cardiac arrest time. This was a highly successful procedure that demonstrates the importance of quickly assembling a multidisciplinary team when dealing with highly complex surgery.”
[1] Aortic dissections are divided into type A and type B: Type A occurs in the ascending aorta which is closer to the heart; if a patient of this type does not receive treatment in 48 hours, the mortality rate can reach 50%. Type B refers to a tear in the descending aorta, mortality is comparatively lower as it is located further from the heart.